Why You Need to Start Looking at Your Mid-Revenue Cycle for Lost Revenue

Originally published on Becker’s Hospital Review: https://www.beckershospitalreview.com/finance/why-you-need-to-start-looking-at-your-mid-revenue-cycle-for-lost-revenue.html
By: William Chan, CEO, Iodine Software
84% of healthcare leaders believe the root cause of lost or decreased revenue is inaccurate clinical documentation and coding.* But the challenge of managing a more accurate mid-cycle is that this accuracy is fundamentally driven by ensuring that the patient’s full clinical picture (as reflected in the evidence) is correctly documented in detail, then fully represented in the codes.
And despite massive investments in documentation/coding programs, earned revenue loss continues to persist — to the tune of $5-11M in leakage for an average 250-bed hospital1.
Where and Why Leakage Happens
The overall leakage problem is a combination of the fact that humans are involved at every step, and that most software is focused only on workflows and not solving any issues that may arise along a given workflow. Why leakage happens:
- There are not enough clinical documentation integrity (CDI) resources to review every case, every day, which is necessary to ensure documentation integrity. Being able to identify discrepancies between clinical evidence and documentation is the first step in minimizing mid-cycle leakage.
- Even when CDI teams are pointed to and reviewing the right cases, there’s a substantial loss of integrity at the point of decision to query. The reason for this is multifold — a lack of competence or confidence, a worry about physician response, or a concern about potential for impact. Regardless, the result is that CDI specialists are frequently deciding not to query even when there is a clear inconsistency between evidence and documentation.
- When the query is written, there are fall-offs both in physician response and agreement rates far in excess of what would be expected given the confidence in the root evidence. The causes here are again numerous: poor relationships between physician and hospital, poorly constructed or supported queries, lack of understanding in the importance and impact of better documentation, and a lack of ease of use in reading, interpreting and responding to queries can all drive down integrity at these steps.
- Finally, there’s an alarming loss of integrity at the coding step. Lack of clinical competency, poor interaction and communication with CDI, and failure to cross-connect the implications of evidence, documentation, and code can all be drivers of lost opportunity at this step.
How You Could Fix This — If Money and Resources Were Unlimited
With unlimited resources, it would likely be quite easy. For example:
- You would provide continuous education and resources to ensure physicians were doing their best to document at the point of entry.
- Then you would review every single case, fully, every single day, during the patient’s stay with only the most qualified, tenured and experienced CDI specialists in the market.
- Then, you’d find the easiest, most seamless way to transmit queries to the physicians in a way that worked in their normal workflows and was a minimal burden — perhaps even a pleasure — to drive quick responses. And you would query everything.
- And then, finally, once everything was coded, you would look at every single case again— and not just for DRG mismatches, but for any documentation opportunity lost…and you would again use only the best retrospective CDI specialists with experience and strong tenure.
However, no health system has the resources to deploy these four strategies, and most legacy software solutions are not even capable of finding many financial and quality accuracy improvement opportunities because: 1) they cannot determine when patient information that is supported by medical data is not written in a patient’s chart, and 2) they cannot perform clinical validation, in which clinical evidence does not support something that has been documented, which increases the risk of audit.
Machine Learning: A New Way to Address Mid-cycle Leakage
As Iodine started further examining ways to stop mid-cycle leakage, we realized that current solutions and technologies did not solve the problem. The objective of CDI is to determine whether the written documentation aligns with a patient’s clinical reality, and this requires more than tools with natural language processing (NLP) alone. Instead, this is where machine learning comes in. Machine learning is capable of considering the entire clinical picture and can make connections and predictions based on learnings from other data including lab results, vital signs, medications, radiology results, and other sources.
Iodine has built proprietary artificial intelligence technology and machine learning algorithms that “think” the way a clinician thinks and emulates clinical judgement. We call this approach Cognitive Emulation.
The result of combining NLP and machine learning technology is a solution that evaluates complex medical data similar to a physician’s approach to diagnosing and treating patients.
Iodine applies physician-like assessment to the clinical evidence in a patient’s chart and leverages previous learnings to more accurately determine the likelihood a condition exists.
Results
We started with Concurrent™ — our first product, designed to increase query rates by prioritizing records that contain inconsistencies between clinical evidence and documentation — all without the inherent limitations of rules-, marker- and NLP-based approaches.
Our customers’ results with Concurrent have been impressive to date:
- $1.5 Bn additional appropriate reimbursement recognized annually²
- $2.55MM additional incremental revenue captured on average (per 10,000 admissions, $6,000 average base rate and 70%/30% med/surg split)²
- 86% of clients experienced a growth in query volume²
- 21% increase in MCC capture volume²
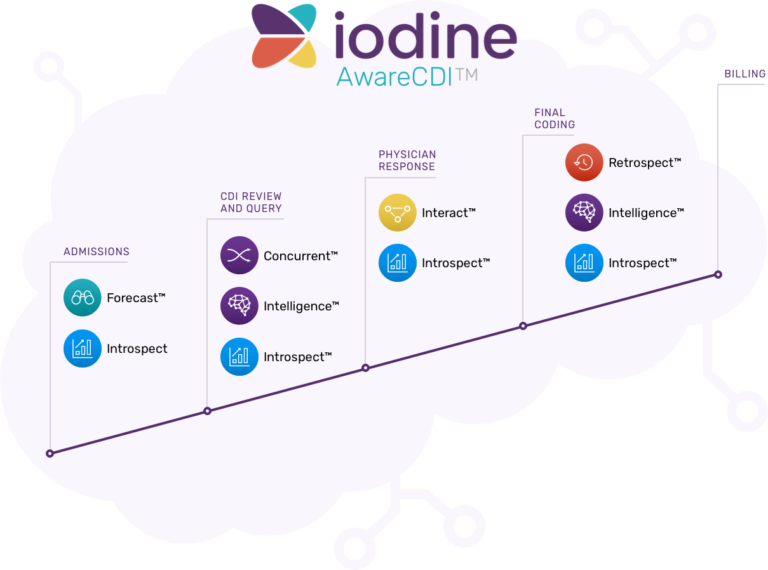
We recently released the AwareCDI Suite to identify and capture additional mid-revenue cycle leakage, beyond the Review and Query stages, all the way through to final billing. You can learn more about AwareCDI here.
*HIMSS and Besler Revenue Cycle Management Research Report- Insights into Revenue Cycle Management October 20
1 2016 ACDIS Advisory Board Study
2 Figures are based on a $6000 modeled base rate and actual measured MCC capture performance from the 2019 Iodine Performance Cohort Analysis of 339 facilities that compared measured MCC capture and CMI impact for the Iodine usage period 9/1/2018-8/31/2019 against pre-Iodine baseline performance.